Telcos successfully embedded within Healthcare remain a rare breed. All the more noteworthy then is BT’s virtual ward & care launch in the UK, spanning AI and digital therapeutics, underpinned by two years’ collaborative preparatory work.
Over that period, we’ve had hints on its Healthcare go-to-market intentions, but have had to wait to see how the promised new strategic direction would scope out.
With no end in sight to the tumult gripping markets, trying to ringfence global directional trends across Healthcare and Life Sciences (HLS) in 2023 is pointless. Scenario planning offers a comparatively better grounding than demand forecasts.
You may feel immune to the course corrections underway within tech innovation circles: the 5G underwhelm; wearables overload; metaverse retreats; SPAC cash crunches; Prescription digital therapeutics (PDTx ) hurdles; generative AI landing out of left field, igniting overnight euphoria.
So what, you say, we operate in the heritage end of the clinical spectrum. And since linear decisions about tech and digital procurement across HLS are atypical, our strategy remains sound enough overall to carry on. It may take longer, but we’ll get there.
You may end up wrong footed. Relying on a single customer base, however compelling your proposition, increasingly leaves you vulnerable to a ‘must win at all costs’ culture, blinkered to alternative routes to market.
The Need for Transformation Finally Dawns
Particularly since Q4 2022 we’ve seen a raft of strategic moves from across HLS: restructuring; C-Suite flush outs; portfolio reworks; unlikely partnerships.
More incumbent providers and life sciences organizations are finally acting on what they’ve known for some time: they cannot singlehandedly offer the end-to-end contexts patients need; and that they must commit to full throttle transformation, or risk disintermediation. For some, there is a lot at stake over the next 5-7 years in relation to R&D, next generation intervention, and commercialization.
In contrast, the pioneering health techs and retail pharmacy go from strength to strength. The strategic investments they committed to as far back as 10 years ago are delivering yet more new service lines, geared to precision.
We’re now seeing credible moves towards end-to-end services in multiple contexts. But this time around there is no competitive land grab. The successful disruptors are already finding ways to innovate with and from inside the HLS system, to work with incumbents to remove friction points.
Convergence Will Underpin The New World Order
And there’s more on the horizon. Convergence is the ultimate target outcome. I dedicated my 2022 predictions to the theme of convergence, underpinned by four interrelated themes:
Strategic Orchestration : Extending the multi-disciplinary and hybrid- capability model across secondary care and its adjacent sectors. This is now also impacting primary care
The Power of One : Cross-functional teams need a common data infrastructure that aligns to their inter-operational evolution
The Curated Experience: The dawn of truly targeted intervention and therapeutics
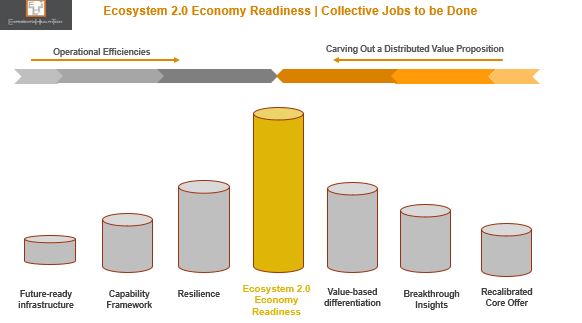
Ecosystem 2.0: The composable-principled ecosystem that can support Healthcare and Life Sciences to align, empower, and transform is only starting to emerge.
I believe that much of what’s currently playing out validates this new foundational model.
Scenario Planning In a Nutshell
Deciding where you (re)position gets more critical with each passing year, as buying power shifts, different services skills are sought, and managed contracts face greater scrutiny.
By considering a range of plausible (but not certain) scenarios, based on market signals of varying strength, you create space for your teams to craft future states, both positive and negative.
Interpreting The Signals
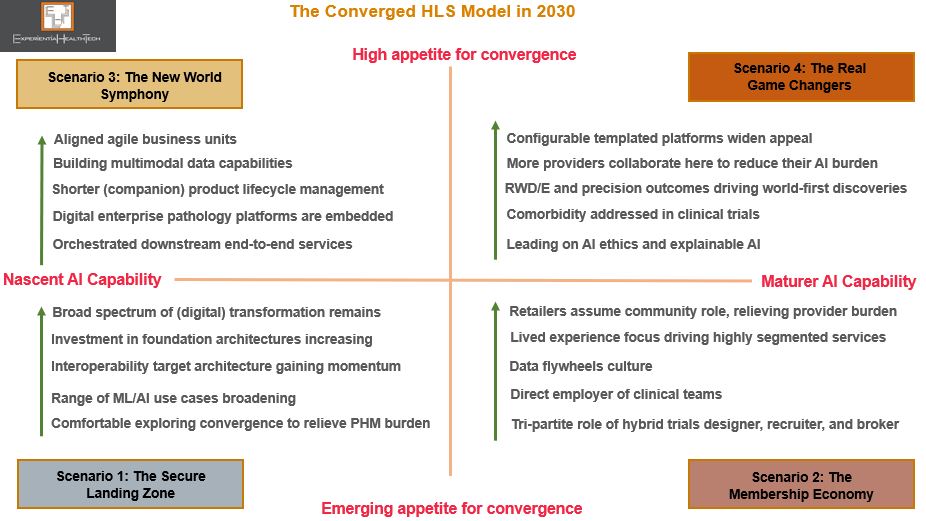
By example, the four future scenarios to 2030 outlined below are framed within two axes: appetite for convergence and AI maturity level – which I see as wholly aligned. Underpinning these are 64 variables.
As we move towards greater convergence, no single HLS sector dominates. Here, the HLS actors evolve beyond their core position, to assume different roles within new configurations:
Acting as a leader in one scenario
Acting as a new partner in another scenario
In fact, within three of these scenarios, there are HLS companies that are outperforming the incumbents.
A growing shift in mindset is resulting in more incumbent leader viewing convergence as a way to remove the burden of innovation from their shoulders, and a strategic accelerant to Transformation.
Here’s some further detail on each scenario.
The Secure Landing Zone
The Membership Economy
The New World Symphony
The Real Game Changers
Scenarios will help your teams not only to assess the strength of your position within each future state, but also to validate, flag up, and steer what you do next in response.
I hope this proves useful. In future posts, I’ll highlight strong exemplars.
If you have any questions or would like to explore further, feel free to reach put to me.
‘Jobs to be done’ will dominate the NHS 2023/24 radar: Clear outcomes; RoI; More of what has supported successful delivery. Tech to underpin weak foundations, boost efficiency, empower.
A tall order, given the new regional Integrated Care Systems (ICS) cluster model is still bedding down. But post pandemic, buyers better appreciate their tech assets. They have a greater awareness of the futility of point solutions, and need for aligned tech and digital investment.
The North Star aspirations don’t disappear, but are de-escalated in the face of more frontline mission critical needs. They’ll also face competition for available budget. The strongest demand potential will come from so-called ‘Arms Length Bodies’ (ALBs) such as the new NHS Transformation Directorate (the merger of NHS England, NHS Digital, and Health Education England), given their remit on national-level futureproofing. However, growth opportunities may be confined to vendor relationships forged through the pandemic.
An NHS Digital Maturity Framework Remains Elusive For Now
If you’re a vendor of US origin, you will likely have been reassured by the partnership between HIMSS and NHS England to co-design a digital maturity assessment framework – recognised internationally, HIMSS provides a solid benchmark on which to pursue and measure excellence. It also helps providers (aka Trusts) to align their investments.
That partnership has been dissolved, with consultancy McKinsey recently awarded a 2-3 year contract to deliver a baseline and an enhanced assessment of maturity across NHS providers and ICSs. Seven pillars will underpin: ‘well-led; smart foundations; safe practice; support people; empower citizens; improve care; and healthy populations’.
NHS England has made several attempts at such an assessment in recent years, yet has achieved very little to-date.
Clearly no-one can wait until this latest project takes off. Common sense alone indicates that maturity levels across ICSs still vary considerably, and will do so beyond 2023. While ambitious and well-led providers have always mapped out their own trajectory, and had the funds to support this, 2023/24 is all about coming together as a local geographic ICS cluster, to audit, streamline, and map immediate priorities.
That of course doesn’t mean that these ambitious providers will stall their strategy while others play catch up. This is an ongoing tension that ICS leaders and their Boards will have to manage.
One Provider’s Innovation is Another’s Foundation
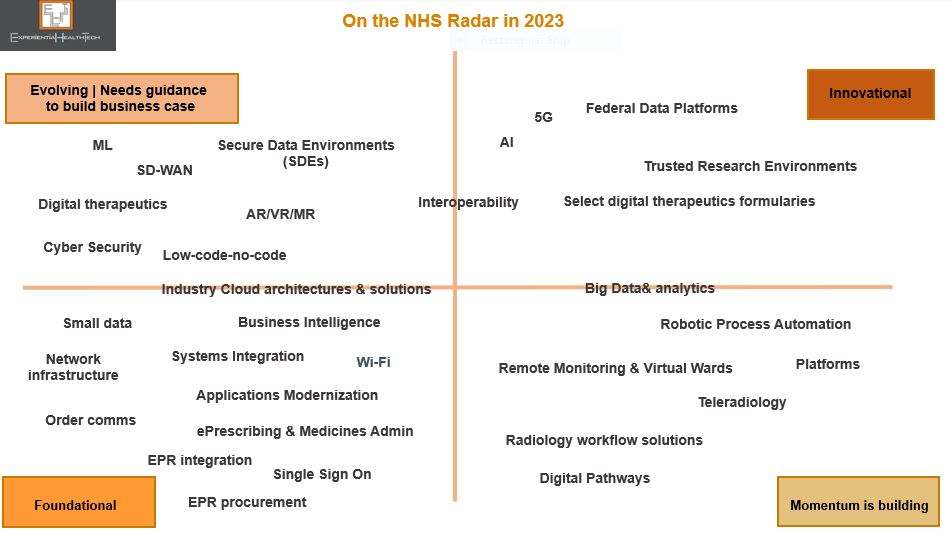
To support vendors on where to direct their effort through 2023/24, Experiential HealthTech has mapped out which digital and technology areas are high priority, and therefore most likely to attract available budget.
These priorities are grouped across four categories, to reflect both the disparity in maturity levels at individual provider level, and the greater need to align capability and ambition at ICS level. The technologies listed below are not exhaustive. We are not implying that tech procurement teams will move in linear fashion from one category to another.
This selection also chimes with those frontline operational targets we believe to be of highest collective priority in 2023: earlier diagnosis, referrals, co-ordinated pathways, patient flow, remote monitoring, and workforce management.
Foundational: Providers at this level are largely playing catch up. Note that dozens have yet to deploy an EHR. Amongst those that do have one, order comms modules may not necessarily be in scope. A lack of modern Wi-Fi infrastructure clearly stalls new OOH models of care and inhibits patient-centric services. Cloud may or may not be deployed – the most likely exposure will be through EHR vendors. Even instances of small data may be alien to many clinical and admin teams at this level;
Momentum is building: Providers making investment decisions at this level have already taken successful steps towards more co-ordinated care, and are looking to replicate early wins, to perhaps address co-morbidity. In these contexts, workflow and patient flow are being prioritised. Recognised gains also include richer data collection at a clinical and operational level;
Evolving | Needs guidance to build business case: More mature providers are looking to align and advance their ambition through deployment of these technologies. They may either be aware of peer success in these domains, or feel these to be a next natural transformative step. Either way, they’ve reached the stage where they need support on relevant metrics to include to present their case to the C-Suite;
Innovational: Those individual providers or ICS clusters poised to take evolutionary steps towards more of an ecosystem model, where interoperability is understood, data maturity comparatively high, R&D relationships a part of their remit, and more widely shared governance is culturally appreciated.
The opportunity for you lies in deciding which part of the maturity spectrum you want to support. Each category above offers scope for elasticity on which tech is deployed, so ground your value proposition. Be specific. Meet their goals. Ditch generic promises. Your ability to adapt is key.
At an ICS cluster level, expectation and need converges in relation to data & literacy, cloud, cyber, automation, and integration. User and IT team experiences so far have been mixed, partly through some vendor hype, so step up support for more granular roles-based education, transparent pricing advice, modernization, and workload migration.
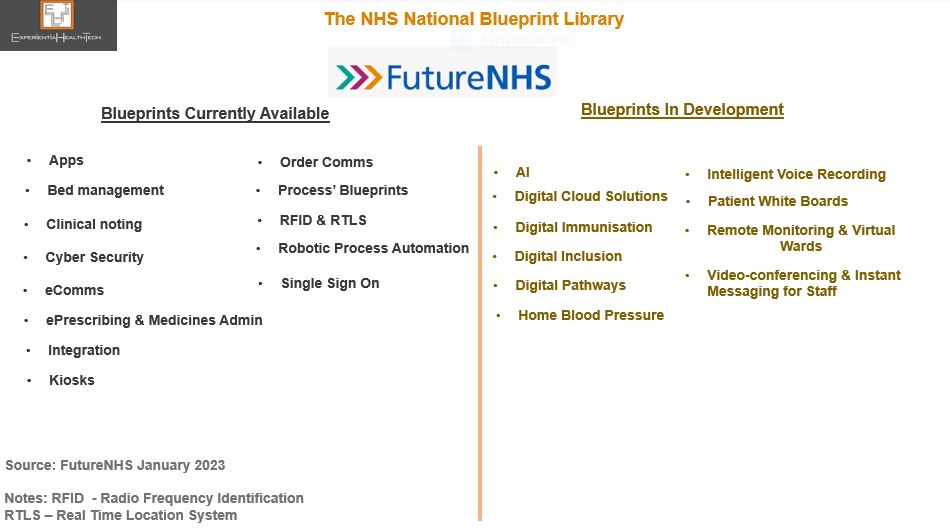
Also worth bearing in mind is the growing peer-to-peer influence via the NHS Blueprints (managed by FutureNHS). Published by providers that have successfully modernised and transformed, they are granular best practice guides. Not all of these blueprints are glamorous, but they clearly illustrate the power of peer influence and gap in transformation and modernisation that’s still out there.
More ambitious tech deployment guides are in the pipeline (see below). Aim to tie in your poster clients here, in context.
One important point to note at this stage is that ICSs are not yet empowered to buy tech and digital as a single buying unit.
Acute care remains the most lucrative demand path, in terms of direct spend, its role as clinical lead on new service models, or partnerships with Life Sciences. Mental health and community less so. Private providers will extend their remit to reduce the NHS frontline backlog, but digital maturity varies greatly here too. GPs are in flux. Social care has yet to line up.
Note that the time to impact buying decisions is shorter this 2023/24 Financial Year, since we have the certainty of a general election by year-end 2024 latest. This mandates a Purdah period, banning new spend from when the election date is announced, until the elected government is in place. That can eliminate six months of activity.
Vendor-Side Jobs to be Done
This ‘sleeves rolled up’ approach applies equally to you the vendor community. Competition continues to intensify, but that doesn’t necessarily reflect a sell-side completely aligned to real world demand.
Incumbents, especially within the clinical software side, continue to add more bells and whistles as a competitive response, without addressing the many enforced workarounds needed to overcome current solutions failings.
Use your current internal cost cutting measures to trigger a reset of priorities, with your partners in tow. Be realistic.
Your pre-sales teams should expect to have to graft harder to qualify leads. Account Managers will need to dig deeper on core and aligned need.
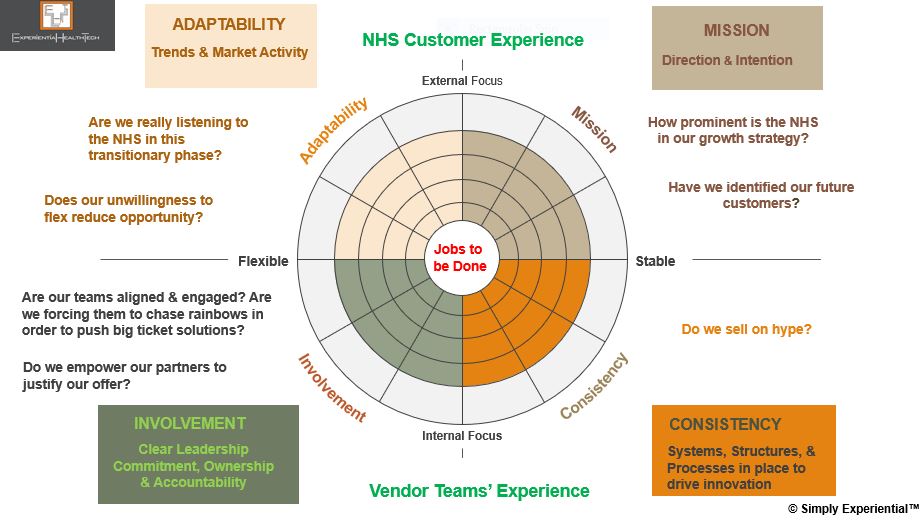
Simply Experiential™ | A Framework for Vendorsand Their Partners
Below are the first-tier components of the Simply Experiential™ framework, which I use with my clients to review the impact of their internal operations on their market success today, as well as their robustness for future-mapping.
It’s a really useful way to bring often disparate teams together, to touch base, strategize, and plan together more effectively.
Your teams and partners explore their beliefs and assumptions about your culture, intention, and context in the market, and assess the spectrum of your capability now and in the future.
While health tech buyers certainly value culture, their loyalty is gained more through a deep-seated commitment to understanding their need at a granular level. Bear in mind that while the vendor and SME community believe they already show this, many experiences shared from across the NHS provider community reveal disconnect, disappointment, and hollow promises.
The framework has more detailed layers, and offers the ability to either hone-in on a specific area that needs to be addressed, or use it to baseline your next steps considerations. Think of it as an anchor to your strategic backbone.
The Bottom Line
The NHS will remain a tough sell in 2023/24. Not all wish lists will be fulfilled. But the tide is turning. With an upcoming general election, it’s natural to anticipate yet further government-led reorganization, especially should a new party get elected into power.
Should the ICS model not survive in name post-2024, its mission will – the NHS has come too far. It’s the many iterations and redesigns over the last decade that have brought the NHS in England to this point. Shaky as it may seem, it’s the best strategic steer we’ve seen, and continues to hold promise.
Effort committed now across your teams will lay down the marker for a greater dividend in the mid-term opportunity pipeline.
When a pioneer and elusive competitor like Salesforce falls from its pedestal, it lands hard. And its leadership is judged all the more harshly.
Perhaps it was always naïve to assume that the co-CEO model, and post-acquisition mergers would be any smoother here. But Marc Benioff has built momentum around ‘Ohana’. This past month has diluted the strength of this culture when pitted against profit.
Although the headlines have been slanted towards the enterprise perspective, its HLS businesses will not be immune, given the strategic direction in which they’re being pulled. Salesforce has been gearing to move deeper into the HLS stack, yet clearly views a single integrated proposition (enterprise bleeding into vertical portfolios) as logical from a cost and profits perspective.
Note that Salesforce has read the markets clearly, and in polar opposite style to the recent move from Oracle, has been delivering a mature response, recognising the buyer preference for hybrid choices to extend capability. HLS can also gain from some of the recent enterprise-side additions:
‘Bring your own AI’, a combo of Amazon’s ML SageMaker and Salesforce’s AI solution Einstein
The ‘Amazon S3 Connector for Tableau’
Blended FHIR and HL7v2 protocols
Aligning Buyer-Seller Ambition
But the HLS buyer lens is narrower. Up until now, each core portfolio offer from the Salesforce stable has been clear cut in its support of meeting their key transformational milestones: Tableau (HIPPA compliant Cloud; Data Visualisation & analytics); Mulesoft (interoperability; EPR integration layers); Slack (collaboration); and Salesforce Marketing Cloud (Patient Experience & Engagement). In tandem, Salesforce has been positioning on Product-Led Growth.
The risk with this shift – which is more than cross-selling – is that HLS perceives such an integrated extensive proposition as overwhelming, or inaccessible to current need and pace.
Case Study | The NHS and Public Sector in England
Salesforce is in the midst of a second attempt to anchor itself across the NHS. Its first attempt was in 2013 in England. However, given the transformational overhaul underway at central and frontline levels back then, it proved challenging for many buyers to clarify their tech needs.
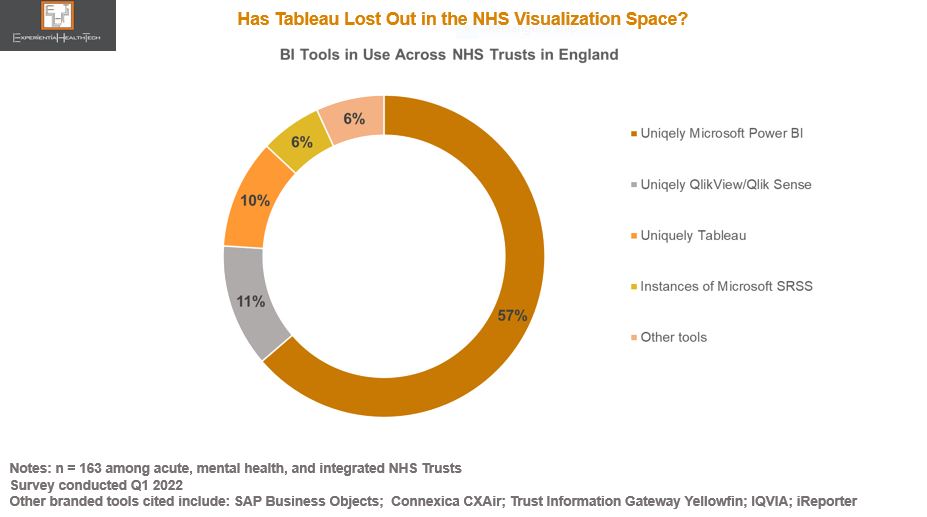
Tableau is an important part of the Salesforce portfolio mix. With data, analytics, and data literacy identified as high priorities for all clinical and non-clinical roles, Tableau is accessible, and therefore facilitates building a business case. But its Account Managers will face a hard graft.
Currently, the Tableau footprint is small at individual provider level, despite the central procurement on their behalf by NHS Digital in 2021: other legacy choices continue, while an ‘Enterprise’ deal struck with Microsoft to include free Business Intelligence instances is proving an obstacle to greater Tableau uptake. Microsoft Teams also penetrated the NHS heavily as a collaborative tool through the pandemic.
In recognition of the challenge, Salesforce is positioning with data driven use cases: workforce management, outpatient flow, screening, patient outreach, advanced therapy management, and drill-down population health.
More encouragingly, Tableau has built a solid relationship with the Open Data and Data Visualisation team within NHS Digital during the COVID-19 pandemic. Although Tableau takes most of the credit for the outcomes achieved – including the donation of the sizeable software implementation – it was once again comfortable working alongside AWS.
The reference above to drill-down population health use cases stems from this relationship. Such was the success, that at one point, 75% of Local Authorities in England were also using the Tableau dashboard on a daily basis, to co-ordinate vaccine outreach at neighbourhood level. A closer strategic partnership between Tableau and NHS Digital appears likely. Migration to the Cloud has been cited as one element on the ‘to do’ list.
In addition, its recent Memorandum of Understanding (MoU) signed with the Crown Commercial Service across the Public Sector may raise the Salesforce profile through buyers’ exploration of low-code no-code capability, alongside access to free experimental project support, and discounted training, among other benefits.
These MoUs are increasingly common across the UK Public Sector, providing one way for vendors to gain more rapid wider-scale accreditation through a commitment to favourable pricing arrangements and access to innovation. It’s not the only procurement channel open to technology buyers – in the UK they can choose from a vast array of frameworks – but it’s good for brand credentials and relationship building.
The Experience Layer Develops
Given the likelihood that Salesforce Executives knew about the planned New Year layoffs. investment in HLS has continued.
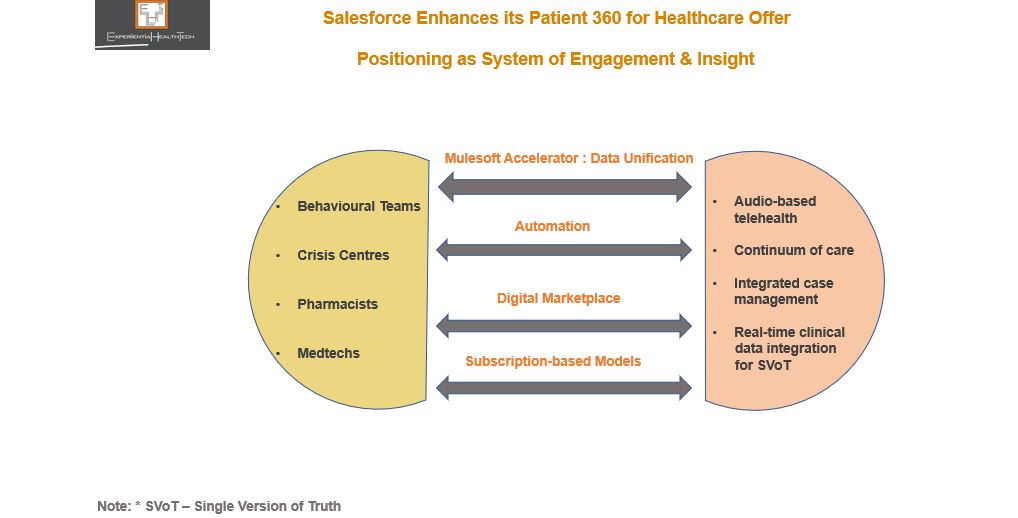
The extent of Salesforce’s HLS ambition was evidenced in November, with the range of enhancements to its ‘Patient 360’ platform, introducing support for behavioural health teams and pharmacists, a nod to the multidisciplinary service model many healthcare systems are striving to develop.
Support for crisis centres shouldn’t go unnoticed either. Although a budget may not be directly available at this level, their inclusion will likely be steered from the sizeable provider or payer installed base already supported by Salesforce.
Charting New Routes to Profit-Led Growth
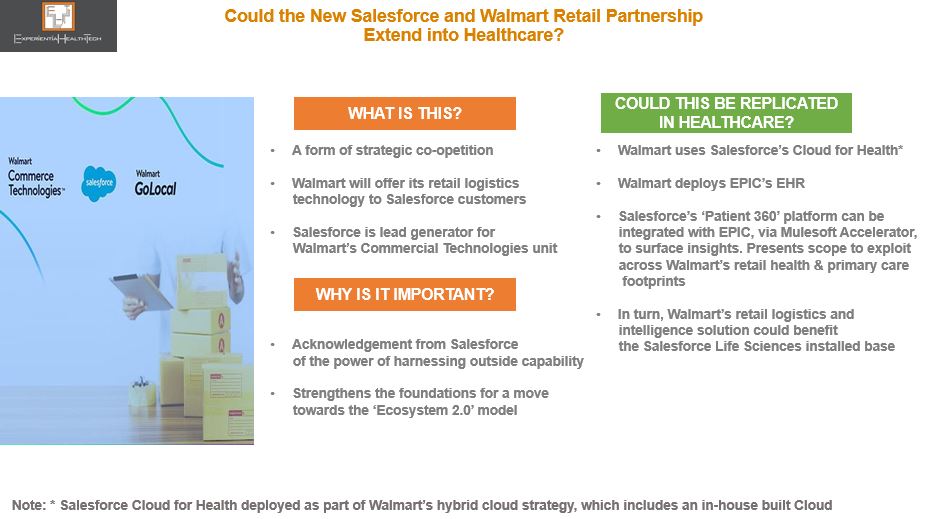
What’s particularly exciting is the newly minted retail strategic announcement between Salesforce and Walmart, potentially carving a new route to exploit ahead of some of its rivals.
Leadership at Walmart has multiple times over proved itself as visionary. The suggestions above in relation to a Healthcare setting may never materialise in this form, but given the ambition of both parties in the US, and the struggles of many of the leading ‘disruptors’ over the last year, this level headed coupling could break new ground.
Walmart’s Commercial Technology unit reflects the confidence to take its in-house developed solutions to the wider market. It’s worth noting too that it already excels at data-driven insight, honed through its loyal consumer-side installed base. With clinical trials the next frontier within retail health, Salesforce could prove a worthy ally for Walmart to accelerate effort here, given its solid footing within Life Sciences.
Salesforce’s Commitment to ‘The Experience’ Will Be Tested
FY2023/2024 is pivotal.
Given its HLS footprint, the pieces are in place to exploit a range of intersectional investment contexts, since provider, payers, medtechs, and Life Science players are each seeking models towards sustainable value based care. Each of these sectors will encounter Salesforce in different contexts.
But Salesforce has also suffered a slew of voluntary departures among key execs from across the business, which may concern prospective buyers and its installed base alike. With ‘trailblazing’ currently not a priority across HLS, neither price hikes nor reduced support will be palatable, as many vendors are already discovering.
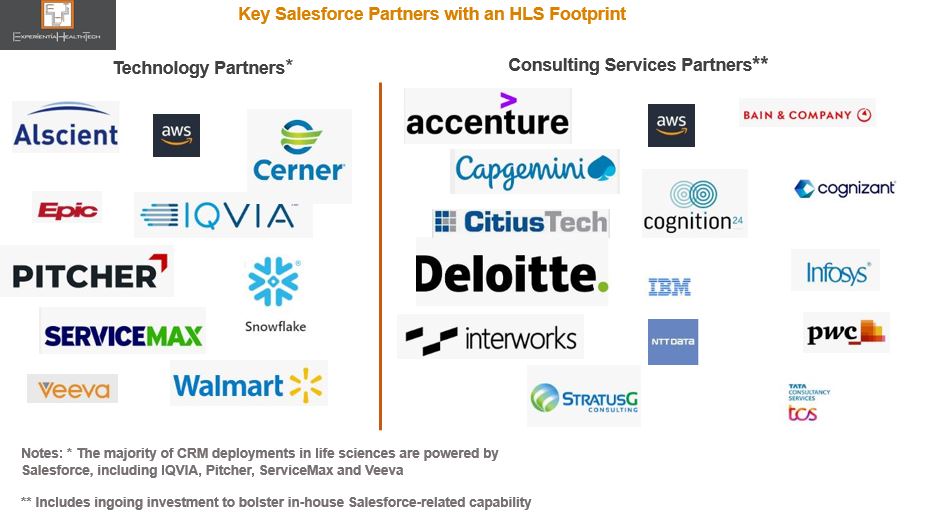
Partners will therefore be key to translate Salesforce aspirations and uphold its commitment – but several are also riding out their own storms.
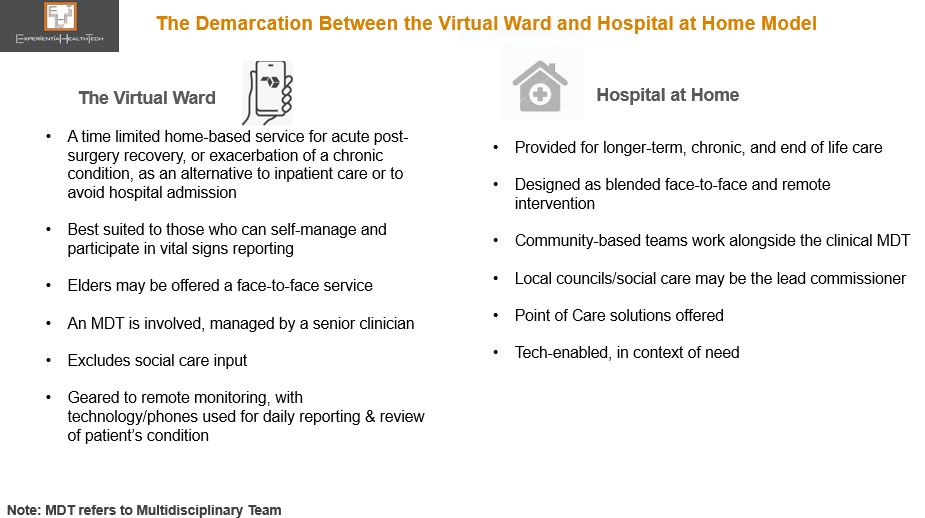
Virtual wards seem a win:win. But some stakeholders are sounding a cautionary note over their sustainability, highlighting the ambiguity about what actually defines a ward. We need to unpick the fundamentals before considering what’s next.
Hailed as a mission critical enabler through Covid, virtual wards, although not new, are being positioned as the common sense answer to many of Healthcare’s service delivery problems. Aligned to ‘RPM’, they offer a clearer context from both the patient and clinician’s perspective, and help frame the service expectation.
But the evidence gathered in support to-date is narrowly confined, relating largely to:
• Earlier discharge of selected patients to continue acute rehab/treatment at home – the emphasis and related costing focusses on releasing hospital beds;
• Wards set up on the fly to deal with covid diagnosed patients – understandably perhaps, cost benefits analysis may be absent.
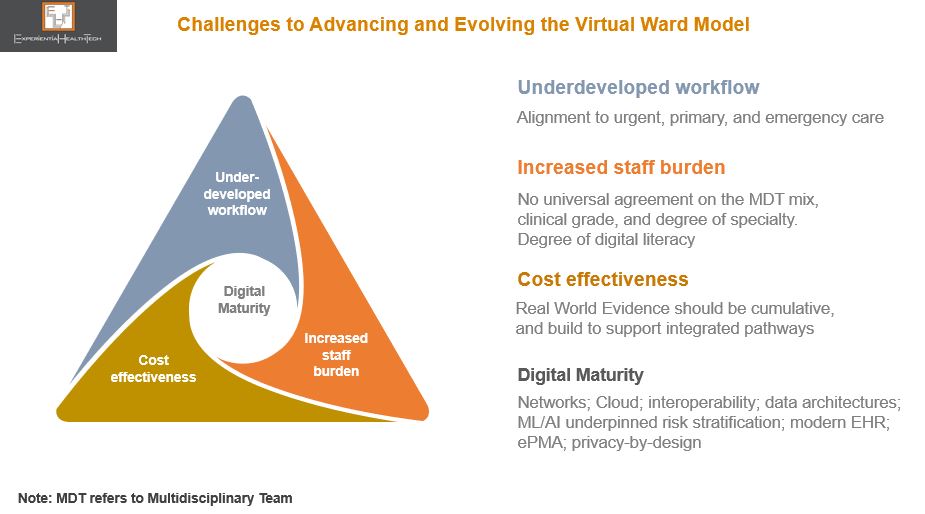
While the more personalised care elements of the ward are attractive, this promise of on par hospital-grade care is interdependent on a robust back end, even before we consider technology. This is as much about patient-and work flow, and outcomes, as it is bed management. And in the overall backdrop of what most Healthcare systems are grappling with, the messaging risks appearing over-simplistic, downplaying the need to pre-plan heavily.
Care From Anywhere?
Post-pandemic, there’s a clear push to anchor this model. NHS England for example wants its 42 Integrated Care Systems (ICSs) to each plan for between 40 to 50 virtual beds per 100,000 population. Indications from the frontline are that this target won’t be met.
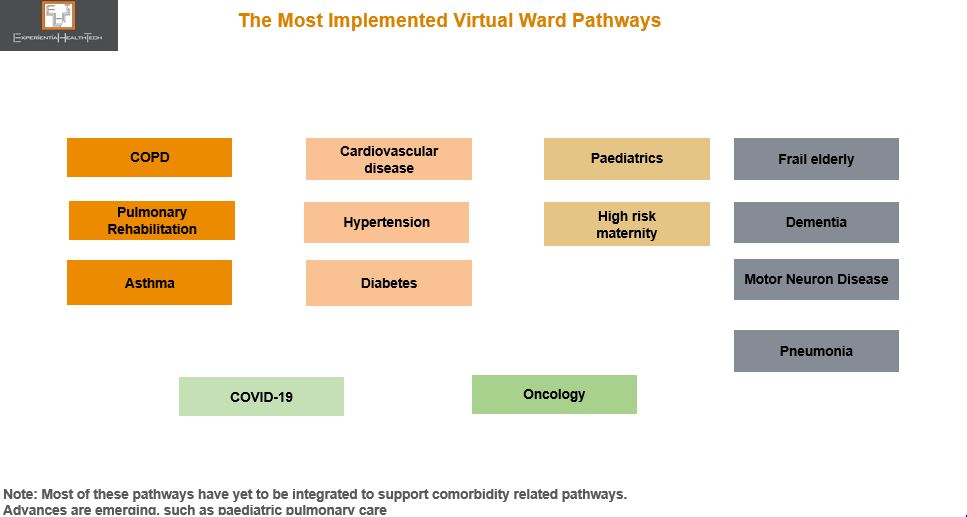
Nonetheless there are NHS success stories, with several providers extending pilots. In July 2022, the Leicester, Leicestershire and Rutland ICS signed Spirit Health, which over time, will implement virtual wards for 16 digital pathways, supporting over one million people.
This is one of the few providers not to position around beds. Plus, it will advance into more complex conditions.
And this reflects the cross roads we‘re at. Virtual wards are critical, but scale-out needs long term aligned local planning, as well as legacy resource and tech issues to be resolved. Wards can’t happen at the side-lines.
Once embedded, they can help underpin the more complex Hospital at Home model. Ireland for example, building towards a tech-enabled reconfigured system, will pursue this route, incrementally building evidence and co-designing with patients from the outset.
The Open Competitive Field is Intensifying
As more providers look to work through post-pandemic backlogs, there is a golden opportunity to win their trust through lower risk pilot studies – which remain the preferred route – but the race to build share is intensifying.
This is about change management. As the competitive field opens up, more vendors are stepping up to support the virtual ward’s evolution outside their core offer, as a way of differentiating. Support addresses governance, digital literacy, virtual ward champions, Allied Health Provider empowerment, UX, patient education, and data planning.
Some vendors are highly credited in other contexts, and through acquisition see this as a natural portfolio extension. Others also offer at-home nursing, tele-health and prescription delivery services. Some are specialist medtechs, while others offer vital signs monitoring equipment, adaptable to a wide range of pathways.
Some are further differentiating through proprietary technology, but operate within Cloud infrastructures. Partnerships are increasingly key, with the likes of Verizon, Atos, and Medeanalytics being signed.
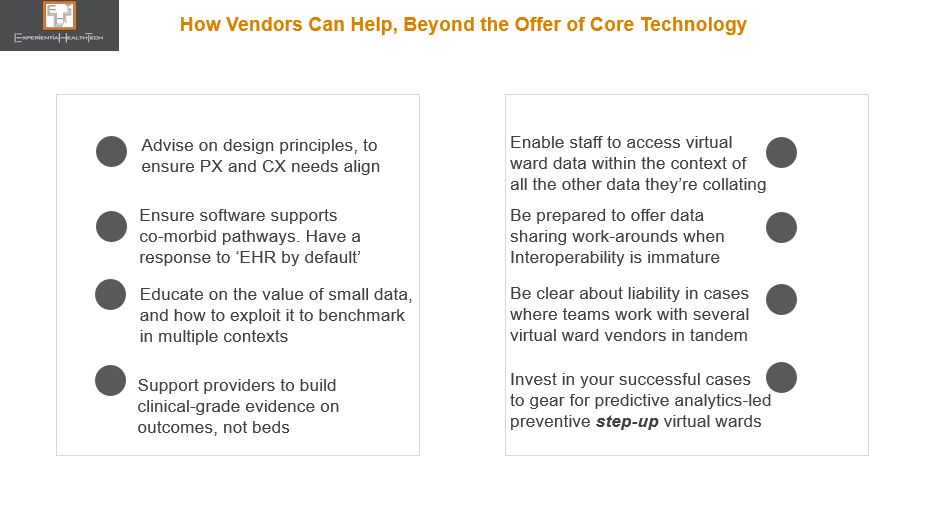
Virtual wards are about so much more than offering a patient kit, or wearables, and vendors should expect to be tested on several fronts.
Those vendors emerging with freshly minted contracts to either scale across a region or across multiple pathways have used co-design to evidence how a templated approach can accelerate the pace at which multiple other virtual ward pathways are implemented, once the foundations are in place. They are setting the expectation for others to match, or surpass.
Virtual wards are exciting, but they must be handled carefully. And as they evolve, we foresee a defined role for newer players such as Pharma to add value.
Below are some suggestions on how vendors can position on value.
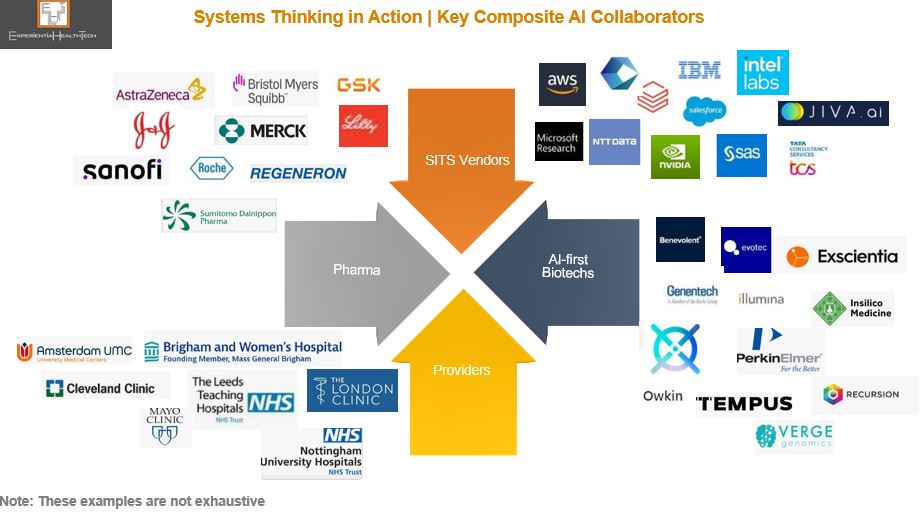
It may be counterintuitive to position AI as an accelerant to precision. And yet an under-exploited paradigm, Multimodal Learning combined with Composite AI, is powering discovery, resetting the benchmark for ‘real world’, and evidencing that precision medicine isn’t a pipe dream. If a broader range of stakeholders across Healthcare & Life Sciences are to benefit, our mainstream conversation needs to evolve. More SITS vendors must step up in support.
We know that a lot of work under the ‘AI’ banner has as many moving parts and shortfalls as it has roadblocks. We also know that embedded within the volumes of good data collected across HLS are swathes of rich but untapped information.
We have reached a tipping point: our current practice of training algorithms from a single modality (e.g. imaging, text, or stats) to validate a tightly defined query doesn’t do justice to our universal efforts to understand comorbidity, monitor disease recurrence, or advance personalised care, and drugs discovery.
There is an alternative aligned approach, with successful field deployment:
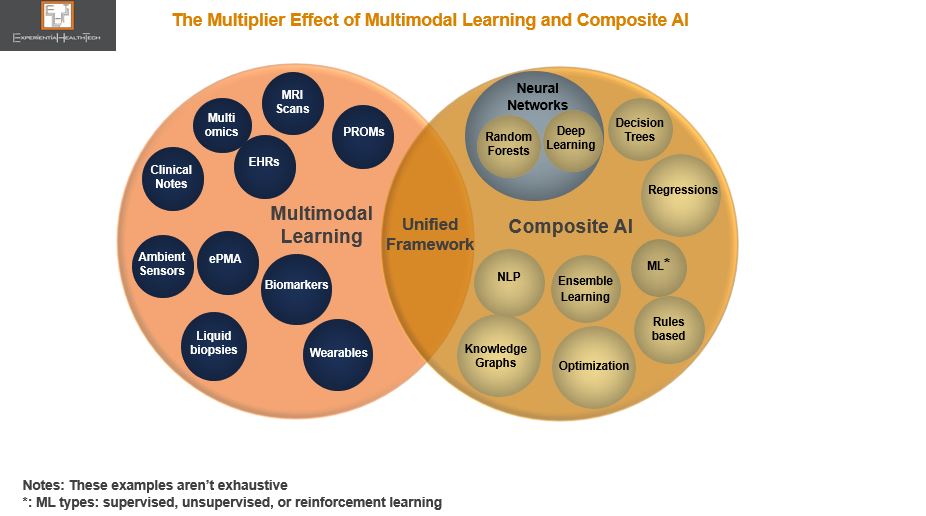
𝐌𝐮𝐥𝐭𝐢𝐦𝐨𝐝𝐚𝐥 𝐋𝐞𝐚𝐫𝐧𝐢𝐧𝐠: Disconnected, heterogeneous (raw) data is harmonised, mined, and then unified into a single model;
The backbone powering this is 𝐂𝐨𝐦𝐩𝐨𝐬𝐢𝐭𝐞 𝐀𝐈, which exploits a range of ML and non-ML techniques, in the context of the specific problem to be solved. This range works together sequentially to ‘fuse’ this data, by disassembling and normalising within one specific technique, before sending it on to another technique to apply further meaning – ‘passing the baton’, in a relay race, if you like. This multi-dimensional approach to tackling real-world problems delivers more granularity and scalability, which has eluded HLS.
Once synthesized, the insight is unified within a framework, which can be shared – several are available through open-source.
Blending The Known Unknowns with the Unknown Unknowns
The sheer range of data that can be exploited may seem over-whelming. However, multimodal isn’t a new approach, with pioneers across HLS already comfortably sharing their respective data with partners to advance.
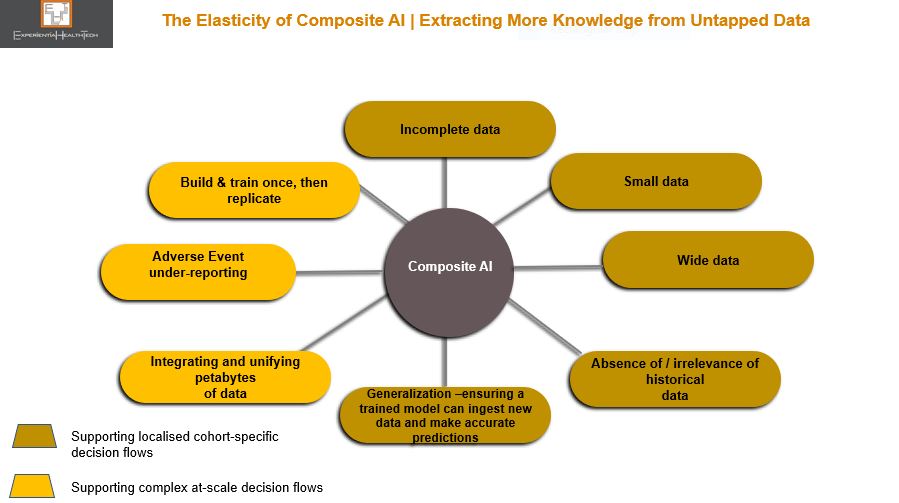
Equally, composite AI may seem daunting, but that need not be the case. The beauty of composite is its elasticity, in that only a few techniques need be applied for greater effect, in alignment to the range of data held, knowledge gaps that need to be filled, and respective skills base.
Acknowledged gains of Composite AI include:
More granular information than RWE
Deeper understanding at a molecular level
Outperforms single modal AI
Embeds Federal Learning and privacy-by-design
Preservation of human knowledge within the loop ‘rounds out’ the data interpretation more deeply, thereby strengthening the analytical process
Users/collaborations add ML/AI techniques at their own pace and capability
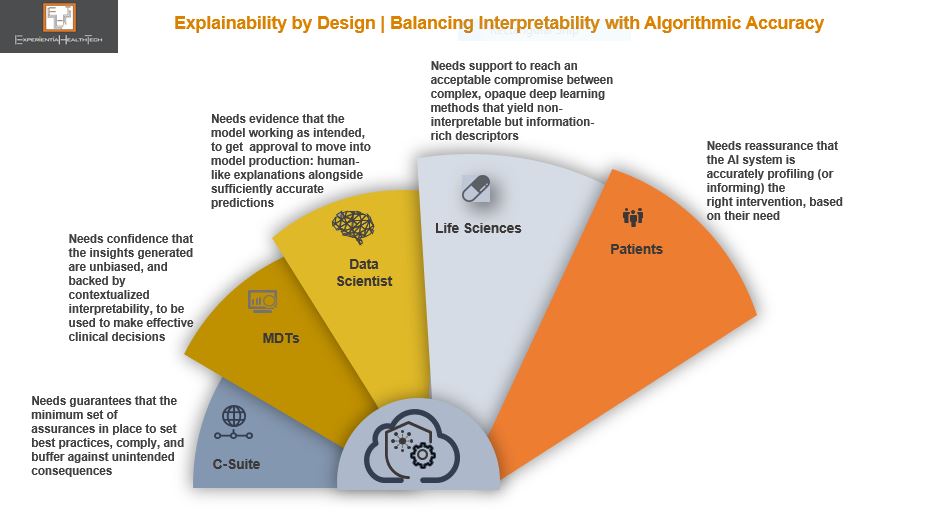
Explainability Versus Interpretability
We may all be familiar with the concept of Explainable AI (XAI), but it’s a generic reference that a whole range of stakeholders, each with differing priorities, are supposed to get their heads around.
This is where the notion of a trade-off in a pragmatic sense needs to be introduced to the mainstream conversation. As we apply some non-ML approaches techniques, which make up the other part of the Composite AI toolkit, in our quest for better detail, the black box comes fully into our front mirror. And we know the level of discomfort this provokes within the HLS community.
While some stakeholders may be comfortable with ML and automation, since these have been widely debated and evidenced, most will not be familiar of the inner workings of a composite model. While these HLS roles don’t need to be experts, there is a strong argument now for at least familiarising them with the basic principles, in relation to those techniques which lend themselves to high explainability, versus those that don’t.
For example, decision trees, which embed graphical representation, can convert data into a narrative of what’s going on. In contrast, Deep Learning, where the model trains itself to process and learn from data, yields low explainability, since the neural networks within are very difficult to interpret.
The trade-off here is whether to accept higher accuracy over single modal AI models, in exchange for less transparency behind the findings in complex data scenarios. We are after all still struggling to strike a balance between the flow of innovation, data fatigue, and actionable insights. This debate will continue for the foreseeable future.
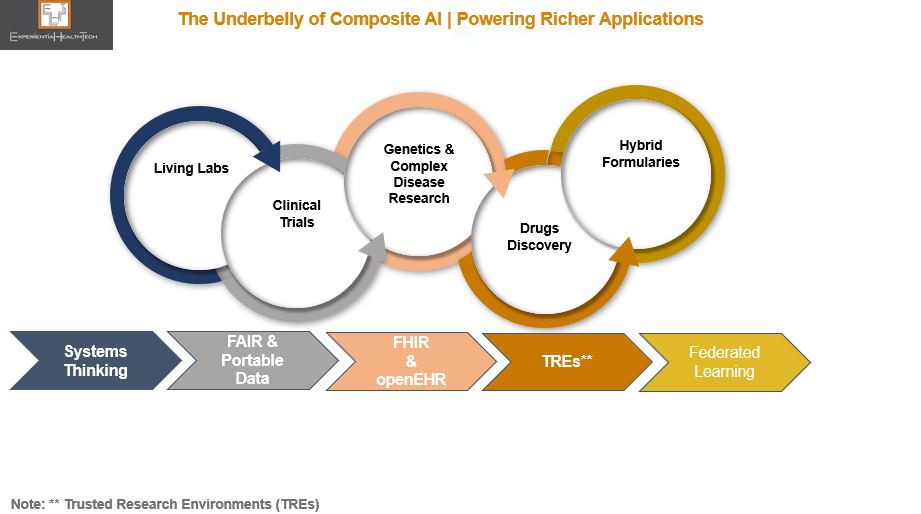
To relieve the burden of ML/AI maturity, this approach validates the need for Orchestrators from across HLS. The growing momentum behind Trusted Research Environments (TREs), systems thinking, and openEHR, across organisations and between research partners, is testament to this. These practices also help to position both Multimodal Learning and Composite AI in a constructive pragmatic light, as multi-disciplinary practices that advance great work among mutually respected peers.
SITS vendors have a role to play here too, alongside HLS teams, to champion the collection of good data, while working to ethics, non-bias, and responsibility. These are challenging but necessary codes of data management conduct that we must instil.
Current composite capability across HLS is already generating richer insight to supply novel intervention. Above are some of the key areas which stand to gain a lot, from healthcare systems such as the HSE in Ireland and NHS in Scotland currently rolling out Living Labs, through to the ongoing collaborative work across clinical trials and drugs discovery. With regulation in more European countries starting to acknowledge and reimburse digital therapeutics, this will, over time, pave the way to capture even more real world data at the edge.
One example is oncology, where multiple projects are exploiting multimodal data in one clinical area, and applying it to another, to better understand the correlation between some comorbidities – powerful stuff. Among these are the many Pharmaceutical leaders shifting their teams’ focus to targeted therapeutics designed for smaller patient cohorts.
Although in many, but not all instances, AI-first biotechs are the Orchestrators, they’re financially supported by a growing number of Pharma partners, via outcomes-based collaborations.
I’ve highlighted the biotech community in other posts as a cultural breath of fresh air. Yes, some parts of the sector are having a rough time at the minute, but there is some brilliant work coming through from pioneers, some of which feature above. The fact that they refuse to form exclusive relationships, yet are highly sensitive to IP preservation has been encouraging more from within the Pharma community to strike partnerships underpinned by Multimodal Learning and Composite AI.
From big tech, SaaS and vertical cloud players have been among the more recent additions to the Composite AI field, and all the signs, including investment, indicate they’re taking this seriously. More providers are joining. And this can only be good.
Composite AI isn’t a silver bullet. More SITS vendors can help to curate, steer, and widen their services offer. Skills support is also a solid way to build customer loyalty.
The Bottom line
We need a move away from the lean diet of ‘ML is doable in single mode; AI is elusive’.
We also need to put our burgeoning information pipelines to much netter use. Composite AI offers an effective path through which to advance at a pace and scale superior to most effort under way today. And while Composite AI isn’t for everyone, it can support multiple current and emerging use cases.
Further, as the concept of Ecosystem 2.0 evolves, Multimodal Learning and Composite AI will attract high calibre members, excited by the potential of what can be achieved together, with confidence.
Once outliers, incumbent US retail pharmacy chains have spent the last 6 years manoeuvring into position as the lynchpin for the Quadruple Aim.
Given the complex make-up of the US Healthcare system, this has been no mean achievement, and should be applauded. Yes, the market is large enough to keep attracting new players looking to disrupt primary care, such as Babylon Health. But Retail Pharmacy already enjoys a solid footprint across all US States, with a rich heritage of customer loyalty.
Its leaders have evolved to the point where advancing deeper into the Healthcare stack with a well-rounded primary care offer makes so much sense.
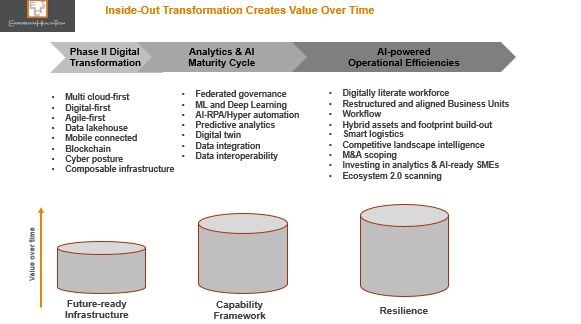
Transformation and the Order of Competitive Play
We talk about Transformation, Digital Transformation, and Disruption as if organizations are hard wired to know when and how to ‘do’ this.
The Retail Pharma sector is transforming and disrupting, with success stories to share. Its leaders have always understood that:
They as incumbents must disruptbeyond their installed base of customers. They haven’t deviated from their core mission – to support under-served communities – yet their strategic announcements through 2022 align to the fact that so many more US citizens fall into this category of ‘unsupported at different stages of their wellness and health;
To disrupt, you first have to define your future today, despite market uncertainties and flux, and prepare every area of your business to pursue this. This may seem counter-intuitive, but by using insight to keep track of headwinds and tailwinds, vision and strategy are better informed, and take out guess work or reliance on intuition.
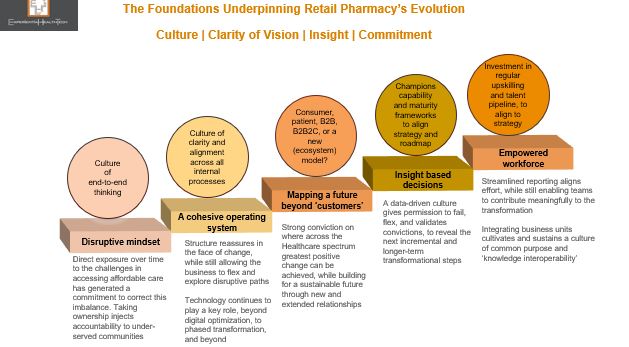
Culture| Clarity of Vision | Insight| Commitment
There are very clear characteristics that set successful companies apart, in any sector. Above all else, the old adage about culture still rings true. Culture is their compass, barometer, and altimeter all in one. Once an organisation agrees its vision and the scale of transformation needed to deliver, culture keeps leaders and the workforce aligned.
Successive Retail Pharmacy leaders within each of the leading 3 US players – CVS, Walgreens, and Walmart – honour these principles.
They are champions of end-to-end thinking: Setting a vision that extends beyond 10 years; being comfortable with not having all the answers up front, yet identifying the customer of the future they want to support, through new service models. Ironically, this mindset is interdependent on openness and evolution, where collaborative solution-building becomes the norm.
Transformation is by nature complex and can never be considered complete. Organisations need a balance of yin and yang to ensure structure and pace. That translates as driving through an internal operational overhaul, to ensure watertight efficiency. This in turn facilitates a meaningful value proposition for the market. In the case of Retail Pharmacy, all roads need to lead to value based care, underpinned by outcomes.
But there are cautionary notes:
Given the installed bases at stake, at-pace scaling mustn’t compromise patient safety. Some investigative reports in the US (outside my remit) claim intense KPI metrics have led to multiple cases of prescribing admin errors. As Europe (currently a digital laggard) gears up for ePrescribing, this aspect will be scrutinised. Trust is precious;
Both Walgreens and Optum Group (now a partner of Walmart) claim to be payor agnostic and champion equity, but have yet to truly reset the status quo on transparency and out-of-pocket expenses. Meanwhile, note the growing momentum behind the much smaller @RosettaHealth and its evidenced framework, delivering eye-watering savings for members.
Insight is Our Oxygen Through Transformation
Insight, based on good data, validates effort when we see small and ongoing positive outcomes. It keeps an organisation’s workforce and partners close to its mission. Analytics and AI-driven insight is intertwined with Transformation.
Experiential HealthTech defines AI in today’s market context as Augmented Intelligence. This not only reflects the capability maturity across Healthcare – embryonic – but also re-enforces that AI will remain a blend of machine and human interaction. This is vital across Healthcare, which needs to keep high touch contexts- as far as resourcing permits.
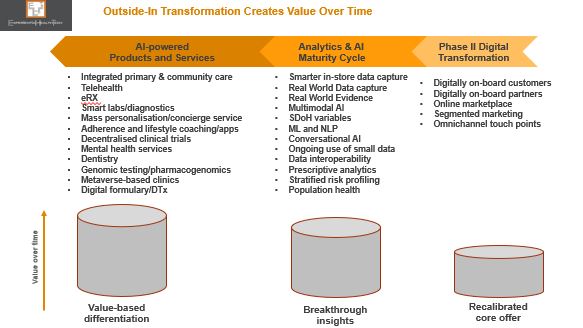
The analytics and AI maturity cycles at operational and market-facing levels are broad, and the pace and scale at which Retail Pharmacy organisations are working through these are dictated by their internal reconfigurations and partnerships.
Throughout the COVID pandemic, one thing became clear: there were petabytes of untapped rich data across Retail Pharmacy. And like other organisations already on a transformation path, radical effective responses could be accelerated, with confidence.
This success will likely have altered Retail Pharmacy incumbents’ next phase priorities: while a degree of competitive overlap remains across their roadmaps, there are also liberal doses of ‘dare to imagine’, with ambition flagged against decentralised clinical trials and pharmacogenomics.
Technology and Digital Blend
Tech partnerships have proved and remain invaluable to Retail Pharmacy. The collaborations being signed, to ensure ongoing enterprise and analytics/AI maturity, showcase how some ‘big’ players are comfortable carving a future-state based on value-driven partnerships and knowledge sharing, rather than ‘fixing’ Healthcare with a land grab. Nor are these retailers insisting on exclusivity – Microsoft, for example is supporting more than one with their ongoing transformation.
These are just some of the few currently supporting the sector.
Healthtech SMEs and AI
SMEs in the form of biotechs, virtual care , and digital therapeutics specialists are contributing significantly across Healthcare. Some embed analytics and other AI modes as a competitive differentiator from Day 1. Many haven’t even started along this road. And yet they must, because we need to end up with SMEs that are part of a wider contribution to society, supporting real world need, workflow and other processes. Point solutions help no-one.
For that reason, the interlinking internal and market facing transformation phases outlined above are just as relevant for them.
Retail Pharmacy leaders’ vision does include greater collaborative SME ventures, but for the moment risk is largely managed and weighted within VC funding, or support to modernise the SME operation as a future-proof.
As their market facing services portfolio continues to evolve and augment the Healthcare-at-Home vision, I expect to see a wide range of SME-related announcements:
CVS, for example, continues to back analytics and virtual care specialist Biofourmis (Series D) – and so a multimodal AI focus may yet emerge to align with CVS’ direction.
In India, Walmart is training 5,000 micro and SMEs (micro enterprises are the backbone of the Indian economy) over a 5-year period. Participants will have access to advanced business tools and advisory support to grow their offline and online businesses. There is an additional potential to advance and gain accreditation through the Walmart marketplace.
This isn’t about conquering: it is about broadening the spectrum of affordable choice, equity, and bridging more of the chasms across the Healthcare system, to enhance local population health. Good data and the power of outreach will remain critical levers. (smaller) Peers elsewhere can copy aspects of this model to start out on their own Transformation.
The Ecosystem 2.0 Economy Beckons
I believe the greatest breakthrough in the US initially will come from a willingness to forge a new model – based on Ecosystem 2.0 – which as composite organisations these 3 US players could orchestrate or contribute to, when the time is right.
In the meantime, the new relationships being forged with payors and their provider networks, Pharma, and SMEs bode well.
Attempts to be ‘patient centric’ still elude many practitioners across Healthcare.
Ironically, it’s the new breed of health tech bellwethers that have grasped patient-centricity (PX) from the outset, and kept it core to every aspect of their mission.
One such exemplar is Happify Health, one of 6 companies I highlighted in my 2022 Trends report “The Year of Purpose-Led Convergence | Vendor Watch List”. From a range of backgrounds, these have been selected for their marked capability to lead and converge with purpose, beyond their core. They have not only recognised the cracks in the current system, but are moving to bridge these through novel approaches. Also recognising that rigid adherence to the status quo impacts on bottom line, relevance, and relationships, they are comfortable working across frontiers.
Here’s what I wrote:
“Happify Health: An evidence based DTx (digital therapeutics) specialist, which has gone from strength to strength within the mental health sector. Heavy investment over the years has enabled it to truly understand buying personas and channels, and to design a portfolio to meet these respective needs. Its platform now supports +50 medical devices and multiple apps.
But here’s the thing: not content with designing a broad portfolio to accommodate varied demand cases, it is now prepping to support acute chronic care instances which trigger mental health problems. There is a significant chasm to cross here, and what it’s proposing excites me.
Happify is also fluent in ‘Ecosystem 2.0’ thinking.” – as defined by Experiential HealthTech.
And so, I’m not surprised about the next chapter, marked by its transition to @Twill.
Simply Experiential™ | Twill in Motion
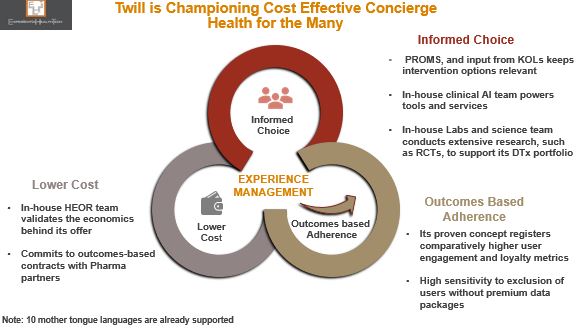
The birth of Twill consolidates its progress over the last 5 years – expanding from D2C to B2B, and the launch of its prescription DTx range – while signalling its ambitious next 5-year plan: to map deeper into an individual’s treatment cycle to offer as bespoke a range of interventions as possible.
Why is this important? Happify has, with scientific evidence, successfully brought together more service components than many of its peers. PX is its DNA: near real-time PROMS data moves with the patient to inform decisions – it has successfully proved that much of the time (but not all), it is possible to circumnavigate the EHR and still exploit new rich data. Individual service users gain directly through deeper engagement and informed choice.
Equally importantly, Twill’s leadership is demonstrating the balanced equation of outcomes-based adherence and lower cost to health systems, Pharma, and payers alike – KPIs with which all Healthcare stakeholders continue to grapple.
There are four new inter-related components which will uphold its future direction.
The launch of Sequences™ | One Step Closer to Personalised Care
The trust placed in Twill by the Healthcare, Life Sciences, and payor communities has resulted in Sequences™, its “end-to-end digital framework”. This translates as a range of modular service options, to reflect the many support contexts typically out of scope among these Healthcare stakeholders, since they’re not operationally geared to configure at this level: evidence-based DTx, well-being products, peer communities, a multi-disciplinary clinical team, and coaching; quick reference, initial diagnosis, short-term and/or longer-term support.
An additional attraction to the partners that have signed up to this is the strong collaborative and co-design foundations on which Sequences is built – providing them with a gateway to new receptive patients and citizens, which have already independently formed trusted relationships with Twill.
But Twill’s biggest differentiator is that it’s one of the few working at the intersection of mental health and acute comorbidity. This is so important, and it’s more than frustrating that more organisations aren’t acknowledging this as ‘the problem we need to solve, together”.
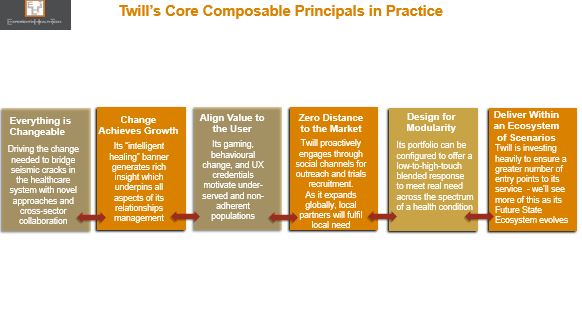
A Look At Twill’s Guiding Composable Principles
Delivery of this model isn’t easy. In my view, Twill has incrementally moved into this position of strength by operating as a composable organisation in all but name. These principals truly embody patient centricity and move way beyond lip service to PX, to deliver a radically improved experience for those living with a chronic condition which is also impacting their mental health.
There are 6 overarching components of composability, which define an organisation’s relationship with its clients and partners, and which form the foundations of the incremental steps they take towards Ecosystem 2.0.
The leadership culture driving composability is the realisation that we achieve more together. Twill is clear that it will not strive to design every solution inhouse, but will happily bring in third party expertise, either directly, or to accommodate third parties already deployed within its B2B client base.
But this will be no loose amalgamation of products. Twill’s portfolio is already of a high enough calibre today to attract complementary third parties, recognising not only the valuable network effect of its open (API-driven) platform, but also the potential of a more rewarding future: migrating away from point solutions to offer a model that not only resonates with service demand gaps, but also chimes with the new forms of clinical workflow and patient flow that we’re crying out for.
That is why Experiential HealthTech classes Twill as an Ecosystem 2.0 orchestrator.
Ecosystem 2.0 with Twill in Outline
The model outlined below reflects where Twill is today (Layers 1 &2), and how potentially it could start to orchestrate its ecosystem (Layer 3). What’s exciting is that new ecosystem members will also steer, contribute to, and govern this future cross-sector state.
Localised members will also respond to local need, and help to accelerate the rate at which Twill can scale, globally, as is clearly its intention.
Federations of secure data exchange
With the permission of its service users, Twill has already built up an enviable rich data set. As its ecosystem grows, the potential to incrementally enhance its clinical AI base is immense – evidence garnered from clinical trials alone, to steer prescription therapeutics, is exciting.
But this is a two-way street. All ecosystem members must commit to Twill’s federated data underpin. Outcomes data from referrals to third parties must be shared back with Twill – to monitor response rates to this intervention, but also to enable Twill to suggest alternative treatment if low outcomes are registered. All of this data creates a SVoT (single record) per service user, and bolsters Twill’s longitudinal system of insight. Population cohort support is also planned.
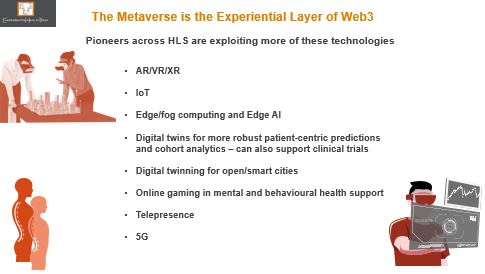
Below is a snapshot of some of the technology investment Twill has committed to. And of course this carries the potential to augment its reach. You can see how this lends itself to Ecosystem 2.0.
This is the future. Not for all of us. But for very many. Experiential HealthTech looks forward to seeing what emerges next from Twill.
Healthcare and Life Sciences (HLS) leaders have dug a lot of deep holes for themselves. Could Web3 yet prove their saviour, and diminish some of their self-inflicted and our real-world problems?
At this point in the ‘digital revolution’, it’s worth reminding ourselves of the many unresolved ‘bread and butter’ issues – taking the shine off what has been achieved. Too many remain unable or unwilling to get closer to the ‘what good looks like’ model we all keep talking about.
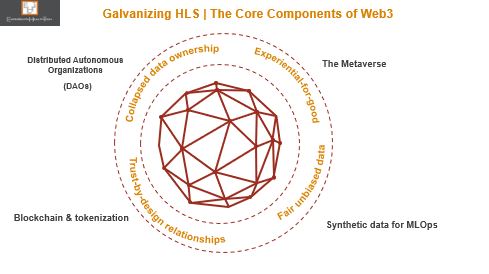
Pockets of pioneering HLS have over the last 7 years successfully notched up a range of use cases that exploit several of the core components of Web3, in all but name – the loose reference to it as the next evolution of the internet doesn’t do justice.
There’s a lot of hype surrounding Web3 at this point, with the wide range of accompanying definitions only adding to the confusion.
But this is far from a fad. And in my view, the HLS community is one of the verticals that can build a solid business case to embed many of its core concepts.
The Metaverse | So Near Yet So Far for HLS
The metaverse has already passed the ‘so what’ test among pioneering providers and life sciences organisations, with deployment in the field for some 7 years now.
Investment has been made across a range of hybrid novel settings: to explore; test & validate; benchmark; educate; and move beyond our legacy ‘one size fits all’ intervention model.
Yet today’s installed base is only really scratching the surface in terms of what could be delivered. Most likely is that exploration and uptake of these sub-components will continue to be incremental, while operational and clinical models continue to reconfigure, evolve, and mature. And let’s be clear, no-one is waiting for 5G to drop before they set out along this path.
The real sustainable benefit of Web3 will come from the bringing together of these ‘proven’ elements, along with others yet to be fully explored.
What Exactly is Web3
Web3 ultimately isn’t so much about the technology implemented, but the art of the possible. It provides a platform through which to pragmatically and simultaneously resolve many of today’s challenges – especially those cultural ‘brick walls’. To quote Sun Tzu from ‘The Art of War’: “Supreme excellence consists of breaking the enemy’s resistance without fighting.”
Alongside the metaverse, blockchain and tokenisation has been making inroads within pockets of HLS – although at a comparatively slower rate. For good reason however, and my view is that the grounded pragmatic examples coming through here will help to convince other cautious or sceptical peers of its validity.
But to my mind the two greatest jewels in the Web3 treasure chest are DAOs and synthetic data. Hand in glove, they offer those within the HLS community the first real opportunity to get ahead of the innovation and discovery curve, instead of chasing their tails.
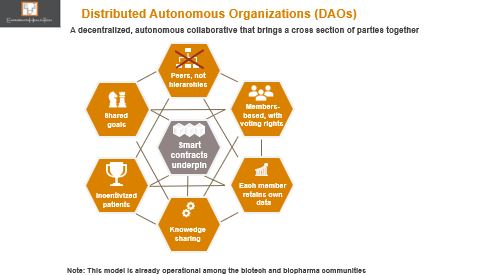
DAOs are the Wrap Around to Web3’s Success
With the interoperability war raging against many of you incumbents right now, and serious efforts to get more HLS stakeholders to collaborate, while pressure mounts to redesign the patient engagement model, Decentralised Autonomous Communities (DAOs) could really strike a chord.
I view DAOs as a more formalised type of the Trusted Research Environment model that’s being actively encouraged within some of the pioneering health systems. DAOs by nature will offer greater scope to integrate a broader range of stakeholders into a community of practice: removing so many of the barriers and uncertainties on how to progress together, within tightly governed parameters. DAOs will add to rather than derail effort to collaborate, and will help to see the wood from the trees in settling clear obtainable goals.
More meaningful relationships could also be nurtured with patients, who, encouraged by the open door a DAO membership offers, would be more likely to sign up and fully participate.
All you health tech incumbents should note that you too can play a meaningful role here. Those among you whose work straddles providers, medtech, and/or life sciences will have more options to consider over the longer-term.
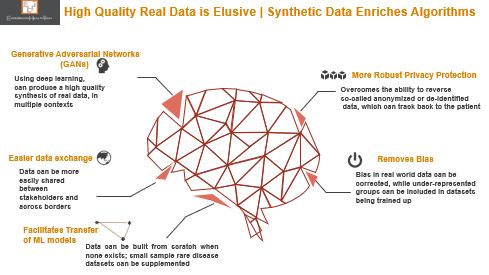
Access to Real World Data is Limiting | Let’s Synchronize
Nearly every conversation across HLS these days involves data – what good data looks like; where to get hold of it; how to exploit it for insight; who owns it; how biased it is.
We’re all aware of the many contexts and settings across the HLS landscape where a data strategy is not a leadership priority or capability; where good data isn’t being captured; where good data is being hoarded; where analytics skills are poor.
The more HLS matures, the more leaders realise they need good data. We’ve now reached the tipping point on fit-for-purpose data. The outstanding challenges in basic data capture and accessibility leave us no nearer to population health.
Enter synthetic data.
And yet the proven benefits from the field in creating synthetic data, if more widely understood and deployed at-scale could be a seismic catalyst for positive change across so many fronts.
Already being used in pockets of life sciences to bolster trials, it’s gaining momentum as a safe accelerant for predictive care. It’s accredited with the same statistical and business value as data collected in the field, or to supplant when real data isn’t available, or when such data is scarce, yet it carries no risk of being traced back to the real source.
One of the most obvious and potentially far reaching use cases will be in the field of digital twins: creating synthetic (proximal) data to mimic certain characteristics of a person, and use this as a blueprint to create a generic model that can be applied in other context.
Web3 could help generate a completely new data continuum, a gift that would keep on giving, locally and internationally.
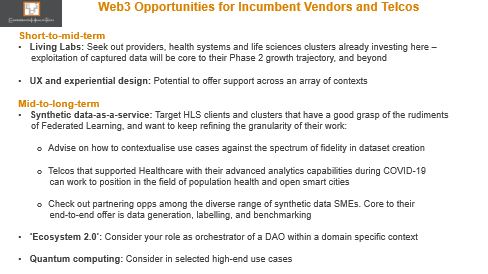
Health Tech Vendors Must Start Planning Now to Support Web3
Yes, Web3 is in its infancy, but it points to a solid opportunity for incumbent vendors and telcos to pursue beyond hyped ‘trends’. That’s why it makes sense for you to get involved in some way at this grass roots level, and identify your entry point.
I’d advise you start planning for this alongside your Business-as-Usual. Because not only will it determine some of your future customers; it will also clarify how you’ll need to upskill your teams; the new types of partnerships to invest in; the lines of business to add; new incentive programmes.
New Web3 competitor types are emerging, not necessarily familiar with HLS. Closer to home, those currently stealing a march are cloud leaders with an HLS footprint, biotechs, and the new breed of health tech bellwethers – culturally geared to operate in ‘future-ready’ mode.
But this is not a gold rush – your effort will deliver both short and intermediate wins while Web3’s infrastructure matures, and momentum builds.
There are also several weak aspects of the model that could dilute the core mission of Web3, to honour the voice of diversity – see below. In most of these areas, an answer lies in your hands.
And if you’re unsure or sceptical at this stage, check out below the growing list of names coming together to form Web3- and related standards consortiums.
The Bottom Line: Interoperability is all over the Web3 value proposition. If you’re not already making moves to at least commit to this in the day-to-day, then this ship will pass you by.
I’ve been lukewarm to the blockchain push in Healthcare, and sceptical on its positioning as a gateway to interoperability.
Despite some success, we’ve not seen anything like the groundswell projected. Was blockchain considered a step too far, or a nice to have ‘icing on the cake’ when in reality the cake hadn’t yet been baked?
And yet, Q1 2022 has been marked by a few noteworthy alliances – looking at the bigger picture through a pragmatic lens, without sensationalism.
‘Noteworthy’ given the names involved. One is Nokia (with its Bell Labs R&D arm) and Equideum Health – formerly blockchain specialist ConsenSys Health, led by the experienced Heather Leigh Flannery, ex-Hashed Health.
Today it’s at pre-launch stage, initially US-focussed, so I’ll return as it evolves, as I still have questions.